ELECTROLYTES
This is going to be a hot mess. Get ready. Also, I'm going to be writing the ranges over and over. And over. And over. Because it helps me remember.
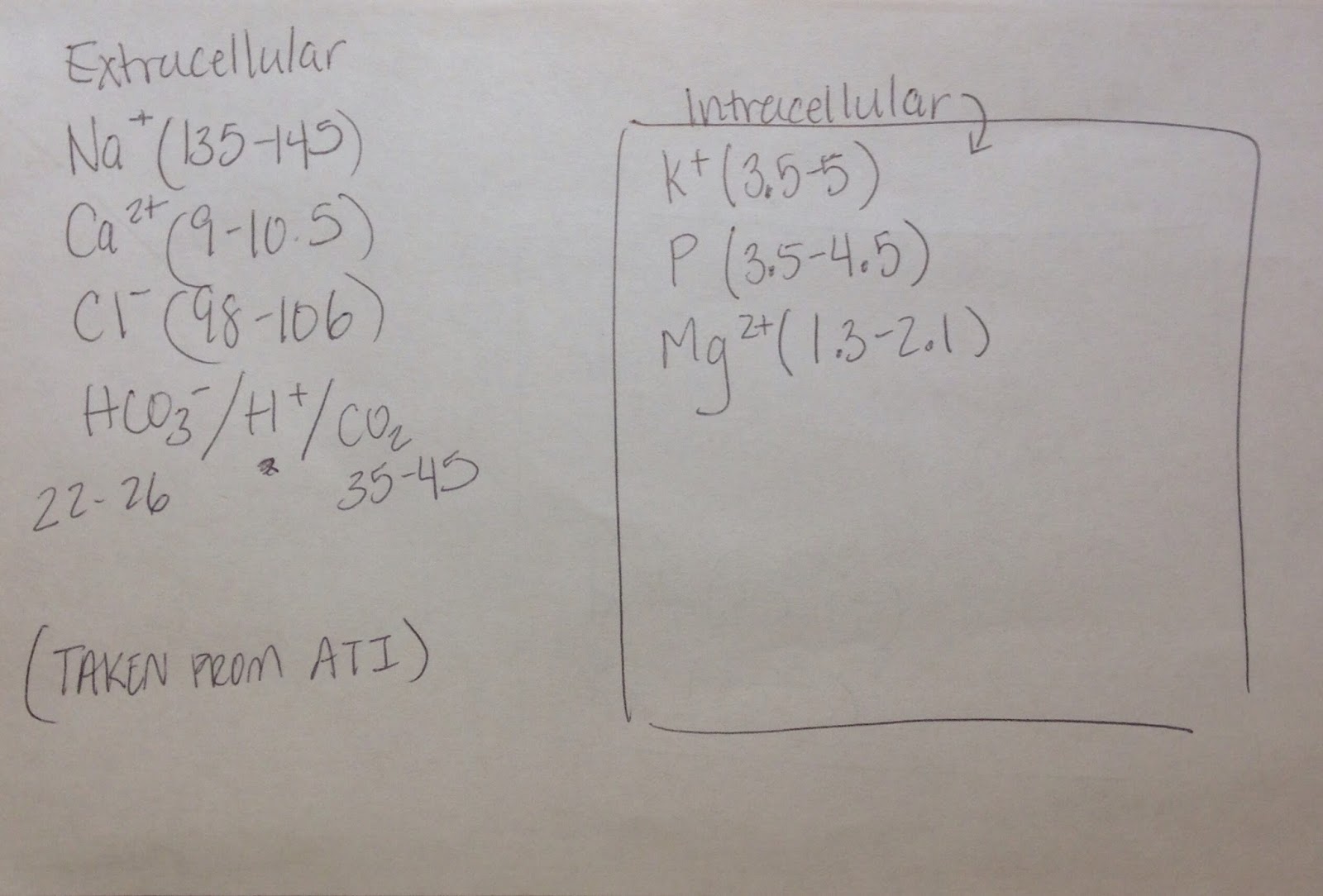
The thing that people forget about electrolytes is that aside from needing certain levels to be balanced, some of them are mostly on the inside of your cells and some of them are outside of your cells. You also have to remember your basic chemistry, which tells you that not only do concentrations matter (diffusion), but charges also matter (like charges want to repel). Cells also have electrolyte specific channels, and perpetually leaky channels, and voltage gated channels...
Here's what happens with nerve conduction:

Here's what happens with myocardial contraction:

Do you have to memorize all of that? No. But the skinny is: At resting, the inside of cells are negative and you need to become positive enough to have an action potential that will send a signal (release neurotransmitters for neurons, or to contract for myocardial cells). When these electrolyte values:
hold true, then, things are in balance. If they aren't, can you guess what will happen? You don't have to memorize all these individual facts. Just think about the cell.
Just remember: K+ repolarizes

Hypokalemia (K+ <3.5-5): Potassium naturally leaks out of cells, keeping the inside of the cells a negative charge. If you don't have enough potassium to leak, the inside of the cell remains too positive. Threshold is achieved, the nerves fire constantly, so it makes sense that a person will feel:
- muscle cramps (your skeletal muscle nerves keep firing)
- confusion/irritability (your brain is overstimulated because the neurons keep firing), leading to nausea and vomiting
- paresthesia (fuzzy fingertips and toes)
- the heart with fire like crazy and in a disordered fashion, and there will be little repolarization, so the T wave (repolarization) will be flat, or inverted.
- and decreased bowel motility
Wait--decreased bowel motility? Why? Remember bowel is regulated by the parasympathetic nervous system. So everything needs to be chill and relaxed for your bowels to move.
You can become hypokalemic if:
- you are taking diuretics (FUROSEMIDE) that make you pee out a lot of K+ (remember, spironolactone is the go to potassium sparing diuretic), or have in general, pissed off kidneys.
- you're on corticosteroids (because they keep Na+, so you have to pee K+ out to balance the charge).
- you're taking digoxin (digoxin competes with potassium at the ATPase pump), its prevents your cells from taking in more potassium (preventing the reset of negative inside charge, so to speak). By the way digoxin reference range is 0.8-2 ng/mL, and the antidote is digoxin immune FAB aka Digibind.
- moderate diarrhea if you're abusing laxatives (laxatives help you excrete potassium, which is why we give kayexalate if you have hyperkalemia)
- you're not eating enough potassium (oranges have potassium).
Treatment of hypokalemia:
- Assess/monitor EKG, I&O, ABG (remember: HCO3- 22-26; CO2 35-45), diet, give oral or IV replacement as prescribed.The thing to remember is, when a patient has hypokalemia and the doctor orders IV K+ NEVER BOLUS! And always check the kidneys. "No pee? No K+," because if you give a person with crap kidney function potassium you could end up with hyperkalemia and stop their heart (see below).
Hyperkalemia (K+> 3.5-5): Potassium naturally leaks out of cells, keeping the inside of the cells at a negative charge. If you have too much potassium, the cell remains too negative to reach threshold.. The nerves won't fire, so it makes sense that a person will:
- Have super tall T waves (super effective repolarization)
- Ventricular dysrhythmias (I'll explain the really cool but horrifying magic in another post), which is such a vague way of saying "you're dead."
- Muscle twitching (your muscles are trying to contract but can't quite go through with it) and paresthesia (same), which can get so bad that you have ascending muscle weakness.
- Increased bowel motility. (Remember, parasympathetic, means, need chill.)
You can become hyperkalemic if:
- You're in complete renal failure and can't excrete any potassium while you're eating potassium.
- You're having extreme diarrhea (you lose base out of your ass, so you become metabolically ASSidic, causing your cells to compensate by shunting K+ out of the inside of your cells and taking in H+ aka acid to save your life).
- You're taking spironolactone, amiloride, triamterene (the most common potassium sparing diuretics).
- ACE inhibitors (no aldosterone=no potassium excretion), and in a similar vein, adrenal insufficiency (which is basically your sick body doing the same thing that ACE inhibitors do).
Treatment of hyperkalemia:
- Assess/monitor EKG, I&O, ABG (remember: HCO3- 22-26; CO2 35-45).
- Reverse the cause of hyperkalemia (neutralize the acid with bicarbonate, get the kidney working again/get the patient to dialysis)
- Give: DW50 with regular insulin, bicarb, calcium gluconate, kayexalate, loop duretics.
- Hold the orange juice.
Next, in the firing sequence, sodium.
Remember, threshold breached=Na+ flood.

Hyponatremia (Na+<135-145): Decreased sodium prevents action potential propogation because there isn't enough sodium to cause the inside of the cell to become more positively charged, so you don't get neuron excitation. It's natural, then that you'll experience
- lethargy and weakness (lack of contractions or signaling)-->confusion, hypotension, headache, seizures (any time you're messing with neurons you're going to get seizures, whether it's too much or too little of an electrolyte)
- the hypotension leads to tachycardia because your heart is trying to compensate for hypotension
Causes of hyponatremia include:
- the body is suffering from a disorder that causes it to retain too much water, such as SIADH, or when you drink excessive amounts of water like during a hazing ritual
- salt loss through excessive sweating (exercise, fever from serotonin or neuroleptic syndrome), excessive urination, such as with hyperglycemia, or accidentally tricking your body into thinking it has too much salt and causing it to pee out the salt, like when you're overdosing on lithium toxicity (0.4-1mEq/L).
Treatment of hyponatremia: restrict water intake, give sodium replacements. I&O/daily weights. Possibly vasopressin to help until you can get sodium levels back up to the right amount.
Hypernatremia (Na+ > 135-145): If your nerves are constantly firing since the threshold is being met, you'll have symptoms similar to those of hypokalemia (not enough potassium):
- hyperreflexia/twitching-->lethargy/restlessness irritability/tachycardia (overstimulated cardiac myocytes)-->hallucinations and seizures
in addition to the effect of having much of the water in your cells get sucked into the blood vessels, which will cause:
- the sticky mouth, cracked mucous membranes (remember all of the water is coming out of the cells to dilute the sodium in the blood stream)
- hypertension-->stroke, pulmonary edema
- fever
Causes of hypernatremia include:
- dehydration (heatstroke, water deficit, diabetes insipidus)
- burns
- GI loss (vomiting, or diarrhea)
- hypertonic tube feedings
Treatment for hypernatremia is: infusion of 0.5NS or 0.9 NS, with oral sodium restriction, and increasing water intake. Usually infusion is isotonic, since hypotonic is VERY RISKY.
 |
| http://www.guitarnoise.com/images/features/capo.jpg |
Yup. That's a capo. Because Ca2+ and PO4^3- concentrations have an inverse relationship. I don't remember why. When I find out, I'll tell you...****
If you're like me, and you're confused about how having less calcium causes muscle to continue to contract when the action potential graphs seem to indicate that having less calcium would cause repolarization to occur faster, and why hypocalcemia is related to longer bleeding times, here are a few caveats about calcium that they don't mention in nursing school that should clear that right up:
1) In action potential propagation, an adequate levels of calcium is necessary to close the sodium channels after the nerve is first flooded by sodium. In other words hypocalcemia allows sodium to move into the cell, decreasing the threshold of action potentials. This leads to a prolonged Q-T interval. Hence, if there isn't enough calcium present, Na+ continues to pour into the cell, causing the nerve to continue firing.
2) Calcium ions bind together Xa and Va factors in one of the coagulation cascades, so if you don't have enough calcium ions, you may have longer bleeding times.
Hypocalcemia (Ca2+ <9.0-10.5)/Hyperphosphatemia (PO4^3- > 3.5-4.5)--with the above caveats in mind, it should then follow that...
...s/s of CA2+<9.0.10.5, and PO43- >3.5-4.5 are:
- hyperreflexia, tetany/ Trosseau's (bp cuff), Chvostek's (facial nerve)
- paresthesia
- dysrhythmias
- seizures
- impaired clotting
and causes for hypocalcemia/hyperphosphatemia include:
- hypoparathyroidism (remember the parathyroids control serum calcium levels)
- decreased calcitriol (vit D)=not enough sunlight, or inadequate consumption of calcium
- pancreatitis (lipolysis as a result of pancreatitis creates fatty acids that bind with Ca2+)
- decreased kidney function resulting in decreased phosphorus excretion and decreased vit D (calcitriol) production.
- multiple blood transfusions (citrate used to prevent blood coagulation binds with calcium)
- alkalosis (causes calcium to bind to protein)
Treatment includes:
- seizure precautions
- calcium supplements/vit D therapy/diet management
- tx hypotension with fluids
- aluminum hydroxide/dialysis/loop diuretics (to excrete phosphate)
Hypercalcemia (Ca2+ > 9-10.5)/hypophosphatemia (PO4^3- < 3.5-4.5):
causes of hypercalcemia/hypophosphatemia are:
- hyperparathyroidism
- Vit D excess, Calcium supplement excess
- phosphate binding antiacids, alcohol withdrawal
- hypomagnesium (stimulates PTH)
- digoxin, lithium (causes intracellular increase of calcium)
- thiazide (causes excretion of phosphate)
- prolonged immobilization (always a test question)
- muscle weakness**
- burns, malnourishment (hypophosphatemia)
s/s of hypercalcemia/hypophosphatemia are:
- hyporeflexia/muscle weakness/lethargy/coma--if this confuses you (and it confused me, because I kept thinking that Ca2+ prolongs signal propagation) it's ok, just remind yourself that more calcium in the blood IS NOT THE SAME AS elevated calcium within the muscle fibers of neurons. In fact, it's the opposite--as in the extracellular membrane is more positive, meaning the threshold is elevated, making the action potential LESS likely, not more. It's ok. Brain fucks all around.
- Hypercalciuria/flank pain/deep bone pain
- Polydipsia/polyuria-->dehydration, N/V
Treatment of hypercalcemia/hypophosphatemia:
- Weight bearing exercise/increased mobility
- Bisphosphates (causes free floating Ca2+ to bind and become bone), calcitonin spray)
- Calcium chealators
- dialysis
- furosemide
Hypomagnesium (<1.3-2.1): very rare. Occurs with poor diet (starvation or alcoholism), increased renal loss due to diuretics.
s/s: neuromuscular and CNS/Cardiac hyperirritability (including Trousseau's and Chvostek's)
treatment: magnesium supplements, monitor ABCs.
Hypermagnesium (>1.3-2.1): Usually only occurs with intake of supplements or medications such as magnesium sulfate for GERD or for (pre)eclampsia treatment in the addition to renal insufficiency.
s/s: neuromuscular/CNS/cardiac depression
tx: calcium chloride or calcium gluconate, furosemide, and dialysis.
****Okay. So according to my friend's textbook from med school, when the serum calcium is low the parathyroid gland responds by releasing PTH, which, increases urine excretion of PO4^3-. Also, (according to Lewis, Dirksen, Heitkemper, Brucher MedSurg 9th edition page 1139) "The parathyroid glands secrete parathyroid hormone....it's major role is to regulate the blood level of calcium. PTH acts on bone, the kidnesy, and indirectly on the GI tract. PTH stimulates the transfer of calcium form the bone into the blood while also inhibiting bone formation, resulting in increased serum calcium and phosphate. Then, in the kidney, PTH increases calcium reabsorption while simultaneously excreting phosphate..." (by this point we're in hyperphosphatemia because it was calcium we were deficient in, but when we started breaking bone down to release calcium, we were simultaneously increasing phosphate levels. So, this is a bit misleading to say that "CAPO, calcium is inversely related to phosphorus." It's NOT that when the body has low levels of calcium it retains phosphorus (or vice versa). It's that, when there is low levels of serum calcium, the body has to break down more bone to create more calcium for the blood stream, and in doing so, there will be excess phosphorus, so the body has to get rid of phosphorus.
No comments:
Post a Comment