 |
| http://www.studypk.com/wp-content/uploads/2015/02/The-Pulmonary-Artery-Catheter.jpg |
Hemodynamic monitoring is the measurement of pressure (PAWP and CVP), flow (CO), and oxygenation (SaO2 and SvO2) within the cardiovascular system, mainly by probes within the mediastinum/heart/lungs. We use hemodynamic numbers to calculate how well the heart is pumping, if the fluid is balanced between the lungs and the heart and the systemic circulation, and whether or not the drugs we're giving the patient are working.
Preload
Right atrial pressure aka the central venous pressure (CVP)=2-8mmHg. This number tells you how well the blood is traveling from the body back into the right atrium to "refill" the heart. If the number is low, that means the blood isn't returning into the heart, and that can be caused by hypovolemia. If the number is high, that means plenty of blood is rushing back into the heart, and that is usually caused by hypervolemia or RSHF.
remember: hypovolemia <CVP=1-8 mmHg<hypervolemia, RSHF
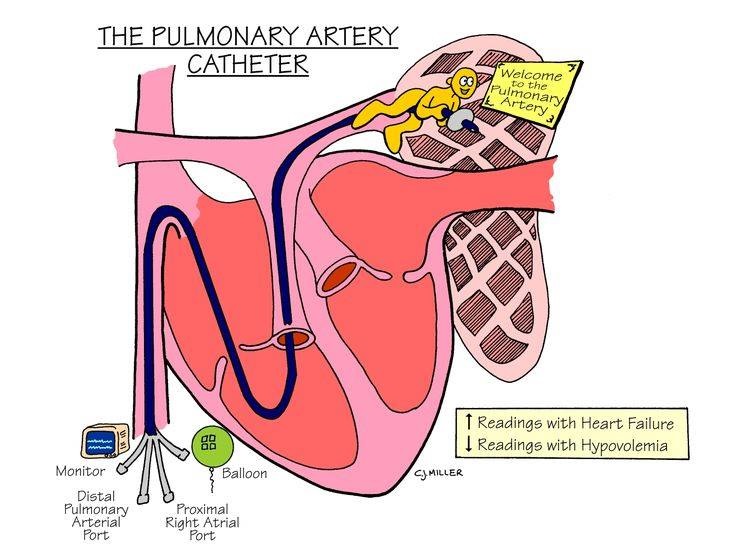
Left atrial pressure aka pulmonary artery wedge pressure (PWAP)=6-12mmHg. This number tells you how well the blood is being pumped to the rest of your body. Technically, this means "the left ventricular end-diastolic pressure." And I used to get confused because this probe is in the pulmonary artery, so, doesn't it technically measure the blood going to the lungs? However, since the blood going to your lungs is also returning into the left atrium, then flowing to your left ventricle (assuming a proper bicuspid) then that blood will be ejected out into the aorta (with the help of a proper seal from a healthy bicuspid). Now, if there is cardiac tamponade, left ventricular failure or hypertrophy the heart can't expand to refill properly. If the heart can't expand or can't pump, the blood will "back up" from the left ventricle, to the left atrium, to the pulmonary circulation into the pulmonary artery properly, right? This results in lots of volume bearing down lots of pressure onto the little PAWP balloon.
remember: hypovolemia<PAWP=4-12mmHg<LSHF, hypervolemia, or cardiac tamponade
If that doesn't make a lot of sense, make sure you go back and review your cardiac blood flow. And if it still doesn't make sense just walk away and come back to it later. This is my 3rd time through this material and I literally JUST had a lightbulb. I've learned to just accept sometimes you don't get something, but if you can remember it and use it properly and file the frustration in the box of "who gives a crap, I know what the number basically means. One day after I've passed the NCLEX it will make sense."
The first picture is a bit misleading, actually, there are two probes, the proximal one (in the R atria) and the distal (in the L atria). See here.
Other hemodynamic numbers you should just know:
CVP: 1-8mmHgPAWP: 4-12 mmHg
Cardiac output 4-8L/min = Stroke volume x Heart Rate
Mean arterial pressure 70-105 mmHg = [systolic + 2diastolic]/ 3
Systemic vascular resistance 1970-2390 gynes/sec/cm^-5= [(MAP-CVP) x 80]/ CO
Arterial hemoglobin saturation 95-100%
Mixed venous hemoglobin (SCVO2): 60-80%
Again, I wouldn't worry about the units.
No comments:
Post a Comment