DIURETICS
The broad brush of diuretics isn't that difficult to grasp. You take these medications, you pee out a lot of water. But there are a few linchpin concepts that are essential for holistic care.
The first thing you have to remember is that with a patient is on diuretics, daily weights and I&O are a must. Remember: "1 pound is a pint," meaning a pound of weight difference is a pint of fluid shift. And also "1 kilogram is a liter," meaning a kilogram of weight difference is a liter of fluid shift. Yes, I know the math is a little off, but those are general rules of thumb. Also apical pulse and BP are vital to prevent a dangerous situation of extreme hypotension <90/60.
Second, you have to remember your electrolyte labs values, because diuretics mess with your electrolytes.
Na+ 135-145
Cl- 95-105
Ca2+ 9-10.5
K+ 3.5-5
PO4^3- 3.5-4.5
And remember what happens to the body when each is out of balance. Preventative safety measures will be necessary.
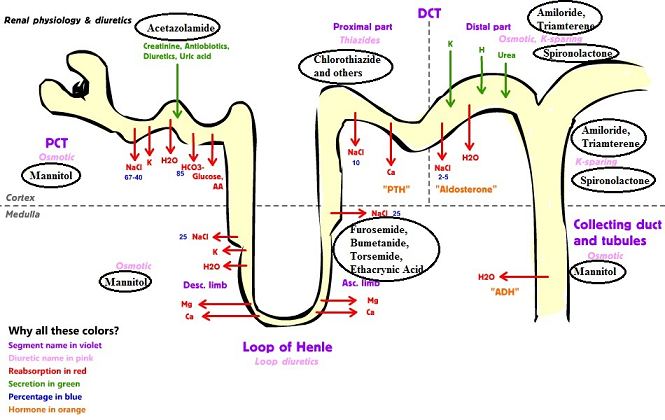
Now let's look at the nephron: Basically, blood comes into the glomerulus, every time your heart pumps. Sodium bicarbonate and the electrolytes are drawn out under the influence of aldosterone, PTH, etc. or retained by ADH, etc. at the proximal convoluted tubule, the Loop of Henle, and the distal convoluted tubule. Then in the descending tubule, the body figures out what it needs to draw back in to remain balanced. The thing that ALWAYS confuses me is that the tubule is where the urine is confined. And the arrows pointing outward from the lumen of the ascending section of the Loop of Henle to the surrounding white area is actually saying that these electrolytes are RETURNING TO THE BODY'S CIRCULATION. Got that? It's ok. I forget it all the time and then confused and cry. (Like, I literally just sat here for 5 minutes flipping from one tab to the other in absolute confusion before I wrote this.) The term "proximal tubule" means the section between the glomerulus and the Loop of Henle, and the term "distal tubule" means the section after the Loop of Henle before the collecting duct (I think).
 |
| https://s-media-cache-ak0.pinimg.com/736x/e7/80/67/e780675385d88cd1fe507bc885c5072e.jpg |
Thiazide diuretics (hydrochlorothiazide, and metolazone): hydrochlorothiazides are one of the cheapest, most commonly prescribed diuretics in the U.S. They block the reabsorption of NaCl, and K+, and therefore water. Metolazone works like hydrochlorothiazide but is much more powerful. It is used with patients with more renal problems but should not be used with patients with complete renal failure (s/s anuria). In fact, none of the diuretics should be used with complete renal failure.
Loop diuretics (bumetanide, ethacrynic acid, torsemide, furosemide): The main purpose of loop diuretics is to block the reabsorption of sodium in the ascending limb of the Loop of Henle. Furosemide (the most commonly prescribed loop diuretic) does this by blocking the sodium-potassium-chloride cotransporter in the ascending limb of the Loop of Henle. If Na+ is blocked from returning to the circulation, water will stay within the lumen. This is why people who take furosemide have frequent urination of large and very dilute amounts. Furosemide also causes renal prostaglandins to be activated. Remember: prostaglandins are part of the body's inflammatory response, and in the presence of inflammation, blood vessels dilate to allow increased blood flow.
Furosemide helps the body to get rid of fluid by preventing Na+ reabsorption, and helps the heart to pump against less resistance by dilating the blood vessels systemically.
All the red arrows showing NaCl returning to the body are shut off by furosemide.
 |
| http://www.mdpi.com/buildings/buildings-05-00405/article_deploy/html/images/buildings-05-00405-g001-1024.png |
- causes excretion of Ca2+ (may be used for patients with hypercalcemia)
- causes excretion of K+ (may cause hypokalemia), which may lead to metabolic alkalosis-- remember, Creatinine check first before K+ supplementation, and NEVER bolus K+
- standard dose for pulmonary edema=40 mg IVP (ask for an order for a foley, if necessary)
- diuretic warnings: orthostatic hypotension, dehydration, falls, take in the AM=no nocturia
 |
| http://www.pharmacology2000.com/Autonomics/Adrenergics1/Renal_Diuretics1u_smaller.png |
Potassium-sparing diuretics (amiloride, sprionolactone, triamterene): K+ sparing diuretics are much weaker than loop diuretics because they work on the distal tubule, and all of the Na+ has already been reabsorbed in the proximal tubule (see above). Spironolactone, the most commonly prescribed potassium-sparing diuretic, works by blocking the aldosterone receptors...
[Recall that aldosterone is a mineral corticosteroid and is excreted by the outer "zona glomerulosa" of the adrenal gland, and is secreted when the body senses a fall in blood pressure. This causes renin to be released by the kidneys, and cleave angiotensinogen secreted from the liver, which is then converted into angiotensin II in the lungs by ACE. Then the RAAS pathway causes aldosterone to be released from the adrenals when signaled by angiotensin II from the lungs, which causes the kidneys to retain sodium and to shunt potassium and hydrogen.]
...which causes the kidneys to excrete sodium in the distal tubule, but to retain potassium and hydrogen.
Triamterene is also a potassium sparing diuretic that works to prevent reabsorption of Na+ in the distal tubules and collecting ducts of the nephron (see image below). It does NOT act on the aldosterone receptors. Triamterene is most commonly used in combination with hydrochlorothiazide (HCZT) because they exert a synergistic effect on the tubules.
Sometimes, the use of potassium-sparing diuretics may cause the client to be hyperkalemic. Remember that potassium leaks out of cells to keep the cell negative. If the concentration gradient prevents potassium from leaking out of the cell to a satisfactory electrical level, the action potential threshold is raised, resulting in decreased action potential propagation. This means your cells will not be easily stimulated, which causes muscle weakness, headaches with n/v, and diarrhea.
 |
| http://biowiki.ucdavis.edu/@api/deki/files/2070/Figure_41_03_03.png?revision=1 |
- don't use salt substitutes (they're made with potassium)
- restrict potassium in your diet (bananas, OJ)
- diuretic warnings: orthostatic hypotension, dehydration, falls, take in the AM=no nocturia
******At this point we're going to take a quick detour to:
HYPERKALEMIA
Should you find yourself in a situation where your patient is hyperkalemic such as:
- potassium rich diet + K+-sparing diuretics
- kidney failure resulting in the inability to excrete potassium
- diabetic ketoacidosis
- burns/gi hemorrhage/hemolysis (eg. tumor lysis syndrome with chemotherapy) or trauma (remember 95% of the body's potassium is within cells)
- infection
Remember that hyperkalemia>6 can cause bradycardia with peaked T waves, so it's an emergency.
The fastest way to buy time is to push the K+ into the surrounding cells using 10 units of regular insulin and D50W to prevent hypoglycemia. In addition, you'll have to give calcium gluconate to decrease cardiac irritation to prevent dysrhythmia. You'll need to do this because kidney or bowel excretion of potassium take hours.
You will have to treat with Kayexalate (sodium polystyrene sulfonate) 30-50 g PO or rectally (if rectal, make sure to check that the patient isn't constipated). Kayexalate exchanges sodium ions for potassium ions in the colon so that K+ is sucked into the colon and then pooped out. Be aware then, that since a sodium ion is being traded for each potassium ion, the client is now at risk for hypernatremia. (I know, it's a pain...) Hypernatremia then causes water to be retained, possibly causing fluid overload. (Ugh! I know!) So, the treatment will then swing back around to excreting sodium and water with furosemide.
*****
And now we're returning to the other two classes of diuretics: carbonic anhydrase inhibitors, and osmotic diuretics.
Carbonic anhydrase inhibitors: such as acetazolamide, work on the proximal tubules where the most sodium is reabsorbed. Normally, with respiration:
CO2+ H2o-->H2CO3---(carbonic anhydrase)---->H+ + HCO3-
carbonic anhydrase breaks down carbonic acids hydrogen ions into hydrogen ions and bicarbonate ions. Hydrogen ions are excreted in the urine and sodium is returned to the circulation, but CAIs prevent hydrogen ions from being split, so the body can't excrete H+ (causing metabolic acidosis), so the sodium remains in the urine and is excreted along with water. Potassium is also excreted.
CAIs may cause hypokalemia and metabolic acidosis.
Osmotic diuretics: mannitol, is a large sugar molecule that pulls water into the tubules. It is used to rapidly decrease pressure in patients with increased intracranial pressure. Because it pulls water out due to osmosis mannitol doesn't cause as much electrolyte imbalances as the other diuretics, and it is safer to use in cases when the brain cells are already stressed by rapid fluid shifts. But, if the client's edema is cause because of hypernatremia, it is better to simply use furosemide, rather than mannitol to excrete water.
Important note: furosemide and acetazolamide are related to sulfonamide antibiotics (like bactrim/septra), so make sure to check for a sulfa allergy before giving these medications.
CARDIAC MEDICATIONS
With all antihypertensive medications you should check the patient for renal function, COPD, and electrolytes/polypharmacy with diuretics. The purpose of B-blockers, ACE inhibs, and Ca2+ blockers are given not only to treat hypertension and decrease workload, but also to prevent heart remodeling from the constant trauma from hypertension and cell death. You always call the doctor even if the BP <100/60 because the doctor will be able to differentiate which medications hold and which to give. Most of your patients will be on multiple diuretics and bp medications.
B-blockers (-olol): So, understanding of the basis of beta blockers is dependent on understanding the sympathetic nervous system. And I'll be the first to admit that I am always confusing which neurohormone does and when and how. The SNS releases epinephrine and norepinephrine from the adrenal medulla in response to stress. Two main organ systems that respond to epinephrine and norepinephrine are the heart (beta 1 receptors with a positive inotropic effect) and the lungs (beta 2 receptors to cause bronchodilation, and in blood vessels to cause vasodilation). Beta blockers block epinephrine and norepinephrine from joining with the B1 receptors, which keeps the heartbeat low, lowering oxygen demand (it also may be used to correct tachycardic dysrhythmias). Beta blockers block the B2 receptors in the blood vessels causing dilation. Sometimes, beta blockers like carvedilol also block epinephrine and norepinephrine from joining with the B2 receptors in the lungs--now this is the brain twisting part: normally, epinephrine causes bronchodilation (hence why albuterol treats asthma). By blocking epinephrine from the the B2 receptors, you unintentionally may cause bronchoconstriction--so they are not suggested for patients with COPD. So, just remember that epinephrine does the opposite things to the heart vs the lungs, and that's may be bad for Airway and Breathing.
Things you should remember besides the bronchoconstriction are: AP for 1 minute, hold Rx if baseline <60 and/r BP <90/60; recheck in an hour. If still <60 or <90/60, call MD.
ACE/ARB (-prils, and -sartans):
ACE inhibs prevent ACE from splitting angiotensin I-->angiotensin II in the lungs, causing vasodilation and preventing the production of aldosterone (preventing the retention of fluids). This is necessary in patients who have decreased renal artery blood flow due to atherosclerosis or antigens OR the heart is failing. ACE inhibitors may cause a chronic cough, but this s/s may not show up for months or years. ACE inhibits may also promote potassium retention, especially with patients on spironolactone, however most patients can tolerate the two medications.
ARB work by blocking the angiotensin II receptor in smooth muscles and in the adrenals. This similarly prevents vasoconstriction and prevents the release of aldosterone. Aside from hypotension, they don't have any major adverse effects. ARBs should NOT be simultaneously given with ACE-inhibs.
Ca2+ channel blockers: Calcium channel blockers don't have a witty suffix for identifying them. You just have to memorize nifedipine, verapamil, and diltiazem. They block the calcium channel blockers in the smooth muscles in the arteries leading to relaxation of the blood vessels. If you remember in the electrolyte post, Ca2+ channels open in cardiac myocytes, increasing the strength and length of contraction, and propagating electrical signals. Blocking these Ca2+ channels will decrease the contractility of the heart and depresse the impulse formation of the nodes, decreasing the heart rate. This gives the heart a better chance to preload, and also decreases the oxygen demand of the myocytes. Verapamil and diltiazem slow down impulse information which helps to control tachycardic dysrhythmias.
Never use Ca2+ channel blockers with acute MI/cardiogenic shock or heart blocks. Know that sometimes CCBs cause edema because arteriole dilation may cause intercapillary hypertension-->fluid extravasation into intercellular space.
Cardiac Glycosides (digoxin): are positive inotropes. They increase the force of contraction and decrease the HR=increased tissue perfusion=decreasing fluid volume overload=decreasing pulmonary edema. Since they decrease the HR, they are also used for tachycardic dysrhythmias. Digoxin is the most commonly ordered cardiac glycoside. Check the AP for a full minute before giving digoxin. Digoxin's therapeutic range is 0.8-2.0 mg/dL. S/s toxicity is yellow halo vision, anorexia, and nausea/vomiting. Remember that potassium and digoxin have an inverse relationship.
Nitrates (isosorbide): dilate coronary arteries=increased blood flow and oxygen to ischemic areas of the heart.
Really Nice Blog, Convatec is a global medical products and technologies company, We providing Like...urostomy bag ,colostomy surgery ,ostomy bag ,ileostomy bag ,ostomy care,therapeutics, continence and critical care, and infusion devices etc...
ReplyDeleteUrine Meter
Diuresis Monitoring system
Closed suction system
Airway management
Critical Care Products