Cardiac Labs
(...with some deviation into kidneys and liver, cause it's all related.)
(Okay, but seriously, I haven't looked at this in 9 months.
This is going to be a beast of a post. Bear with me. Haha, get it?)
This is going to be a beast of a post. Bear with me. Haha, get it?)
Here are the lab values I (you) need to know for cardiac diseases:
Serum electrolytes (in order of greatest numerical range to least, just to make sure I remembered what I relearned yesterday)
- Na+ 135-145
- Cl- 95-108
- Ca2+ 9-10.5
- K+ 3.5-5
- PO4^3- 3.5-4.5
- Mg2+ 1.3-2.1
ESR: 1-13 (the Mayo Clinic says 1-22**)
C-reactive protein: risk for CAD normal <1; average 1-3; high risk >3
PTT: 16-40; aPTT 1.5-2.5X norm
PT/INR: 11-12.5/0.7-1.8 (2-3 on coumadin)
BUN: 10-20 Video on BUN here
Creatinine: 0.6-1.2
LFTs:
- Cholesterol <200
- Triglycerides <150
- LDL <130
- HDL <65
- Albumin 3.5-5
- AST aspartate aminotransferase and ALT alanine aminotransferase 0-35 (signs of hepatitis)
Video on liver function tests here - ALP alkaline phosphatase 30-120 (biliary tree obstruction)
BNP: no failure <100, possible failure <300, failure >300 (300 mild, 600 moderate, 900 severe)
Creatinine phosphokinase MB (CK-MB): <5% (<25 IU/L)
Troponin: <0.2***
*I didn't remember any of them (yikes), so I looked them up in my ATI book. And yeah, I know all of these values are without units, but the NCLEX is not going to try some bitchy unit swap on your to make you fail, and they aren't going to ask you to convert cholesterol units.
** Also, if the values look different, then, well... don't worry that much about it. The likelihood you'll pull the question on the value you don't know is slim, and when you work in the real world, each institution has their own "normal range."
***There's 2 troponins, but my guess is that T is the one used more often because it has the same early detection time (3 hours), but it lasts for longer (21 days vs 10). The other one is Troponin I and it lasts for 10 days and <0.03 is normal.
ECGS
I confess, aside from there being 6 seconds a strip and knowing the general shape of a PQRST I've totally forgotten how to read these. So, let's figure this out together, shall we?
Basics: Strips on the test will come in 6 second sections. Each itty, bitty square is 0.04 seconds of time (you don't have to memorize this). And usually, the strips come with bold(er) lines that outline groups of 5 "0.04 second" sections in 0.2 second sections, like this:

So each "thick gray box" is actually 0.2 seconds x 0.5mV, which matters because:
PR interval should be between 0.12-0.2 seconds (3-5 tiny boxes)
QRS complex should be <0.12 seconds (3 tiny boxes)
You don't really need to get a whole lot more specific than that, except for a few points (like hypokalemia has a flat or inverted T because the threshold for firing has been lowered--but you don't have to memorize numbers for that).
 |
| https://s-media-cache-ak0.pinimg.com/originals/77/9e/c3/779ec32d585f55813ecfd7c8b07f7acf.gif |
The questions you should ask yourself when you look at an ECG are:
1) Is it regular?
2) What is the rate?
- If it's not regular, count the QRSs and multiply by 10 (6 seconds x 10=1 minute).
- If it's regular, I prefer the: 1500/ # of small boxes between two consecutive R-R intervals*
3) Are P-waves present?
4) If the P-wave is present, is the P-R interval normal (0.12-0.2 seconds=3-5 blocks)?
5) Is the QRS normal (<0.12 seconds=3 blocks or less)?
* Why 1500? Because there are 1500 tiny boxes in 1 minute of EKG strip. Prove it?
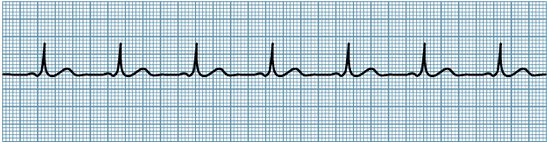
5 tiny boxes x 30 gray boxes x 10 "6 second strips"= 1500 tiny boxes in 1 minute of EKG stripsSo, a normal sinus rhythm:
 |
| http://nuclearcardiologyseminars.com/wp-content/uploads/2013/11/nsr.jpg |
- Regular (meaning, the number of boxes between each R peak is the same-ish): In this case, about 21 boxes between each peak.
- The rate is between 60-100 (remember: 1500/# of small boxes between two consecutive R-R intervals):1500/21=71bpm
- You see a distinct P-wave: Yup, little bump right before the QRS.
- And the P-R interval is between 0.12-0.2 seconds (3-5 blocks): almost perfectly 3 each time.
- And the QRS is tall, and less than or equal to 0.12 (3 blocks) long: almost perfectly 3 each time, also.
Here's a rundown of common dysrrhythmias.
Sinus bradycardia:
- regular
- rate 1500/# r-r interval boxes <60
- P wave present
- P-R interval 3-5 blocks
- QRS tall, less or equal to 3 blocks
Causes: IICP, hypoglycemia, hypothermia, Valsalva, medications (B-blockers, dig, Ca2+ channel blockers), but it can also be a natural reaction to be really athletic or sleeping, so it's only treated with atropine, dopamine, epinerphine, pacemakers, and the existing medications that are slowing the heartrate should be reduced or discontinued if the patient is symptomatic.
Sinus tachycardia:
- regular
- rate 1500/# r-r interval boxes >100
- P wave present
- P-R interval 3-5 blocks
- QRS tall, less or equal to 3 blocks
Causes: physiologic/psychological stress such as dehydration or hemorrhage, angina or general pain, fever, etc., and stimulants, or stimulant drugs like epinephrine, norepinerphine, atropine, caffeine, theophylline, hydralazine, and pseudoephedrine. Treatment: Treat the stressor, vagal maneuvers, B-blockers, adenosine, Ca2+channel blockers, synchronized cardioversion.**
- irregular
- rate 1500/#r-r interval boxes 60-100
- P wave "looks funny," eg biphasic (squiggly looking)
- P-R interval 3-5 blocks
- QRS tall, less or equal to 3 blocks.
Causes: Stress or fatigue, hypoxia, electrolyte imbalances, hyperthyroidism, COPD, heart disease, valvular disease, or use of caffeine, tobacco, or alcohol. This may indicate a reentry mechanism that may become SVT, or enhanced atrial automaticity. Treatment: Beta blockers and cessation of sympathemimetic drugs.
rate: varies
rhythm: regular atrial flutters up to 350 bpm accompanied by slower ventricular regular or irregular rhythms
P-waves are sharp and irregular, giving a "saw toothed" appearance.
P-R interval not measurable because of multiple P-waves.
QRS usually normal.
P-waves are sharp and irregular, giving a "saw toothed" appearance.
P-R interval not measurable because of multiple P-waves.
QRS usually normal.
Causes: Almost always some cardiac disease (CAD, HTN, mitral valve, PE), cor pulmonale, hyperthyroidism, dig, quinidine, epi, which will cause decreased cardiac output and clotting. Treatment: Blood thinners (heparin, then warfarin, slow ventricular contractions if needed with Ca2+ Beta blockers, and electrical cardioversion if unstable, otherwise antidysrhythmics (ibutilidem, amiodarone), and radiofrequency catheter ablation.
Rate & Rhythm irregular, very tiny atrial oscillations that are completely unmeasurable (I don't care what your books says, you're not going to be able to count 600 oscillations). Ventricular contractions irregular
P "fibs"
unmeasurable P-R
QRS usually normal.
P "fibs"
unmeasurable P-R
QRS usually normal.
Causes: multifocal ectopi due to underlying cardiac disease (even pericarditis, and also surgery), tyrotoxicosis, ETOH, caffeine, electrolyte disturbances. Treatment: the priority is to decrease HR *if* the ventricular response is "uncontrolled" or "rapid" (>100) with B-blockers, Ca2+ blockers, dig. Otherwise, if the patient is symptomatic (losing consciousness) cardioversion ONLY IF the patient has be in a-fib for less than 48 hours and/or a transesophageal echocardiogram rules out clots in the atria. If they have been fibbing for more than 48 hours, they have to be on 4 weeks of warfarin (INR: 2-3) before you cardiovert or you could dislodge a clot and kill him or her. Non-cardioversion antidysrhythmic options are amiodarone and ibutilide.
Junctional Dysrhythmias: When the SA node fails and the AV node becomes the pacemaker, and the impulse moves backwards, producing a P wave occurring before, after, or under the QRS complex. P waves appear to be premature atrial contractions.
Rate: regular
Rhythm: often bradycardia (the AV node beats 40-60), but if some SA node impulses occur, it can be higher when the sympathetic stimulation to improve CO.
P waves vary, but often are "invisible" as they are covered by the QRS, and sometimes inverted
P-R interval varies
QRS usually normal
Rhythm: often bradycardia (the AV node beats 40-60), but if some SA node impulses occur, it can be higher when the sympathetic stimulation to improve CO.
P waves vary, but often are "invisible" as they are covered by the QRS, and sometimes inverted
P-R interval varies
QRS usually normal
Causes: cardiac diseases, digoxin, nicotine, amphetamines, caffeine.
Tx: atropine for bradycardic rhythms, B-blocks/Ca2+/amiodarone for tachycardic rhythms.
The AV blocks:
1st degree AV block--Normal rate and rhythm for A&V, normal P, P-R>0.2 seconds, normal QRS
2nd degree AV block--Normal and regular A, slower V, multiple P:V ratio, P-R cannot be calculated since there are multiple P waves, widened QRS. Progresses to complete heart block due to His-Purkinje disease.
3rd degree AV block--P appears abnormal because some will be hidden under QRS--this is because it is complete heart block and the pacemaker that is able to set the ventricular rate is the AV node=severe bradycardia, multiple P:V ratio, P-R cannot be calculated since there are multiple P waves, wide but consistent. Hemodynamically very unstable.
Causes: medication (B-block, Ca2+, dig) or cardiac damage/valve disorders. 1st degree has no real treatment except to discontinue medications if the block is medication related, 2nd and 3rd degree are treated with atropine, amiodarone, and pacemakers.
Paroxysmal supraventricular tachycardia: technically any ectopic anywhere above the birfucation of the Bundle of His, usually triggered by an extra pathway that bypasses the AV node causing a reentrant phenomenon (like with Wolff-Parkinson-White syndrome, which is a type of atrioventricular reentrant tachycardia, which is a type of supraventricular tachycardia--yeah, I know, confusing. You'll get it eventually).
rate: regular
rhythm: Tachy
P-wave: oftentimes obscured
P-R interval: varies if present at all
QRS: usually normal
Causes: overexertion, stress, deep inspiration, stimulants. But also from dig, CAD/rheumatic heart disease, cor pulmonale. Treatment vagal stimulation, adenosine, amiodarone, B-block, Ca2+ block, if hemodynamically unstable, synchronized cardioversion, and radiocatheter ablation.
Premature ventricular contraction: comes from ectopic foci in the ventricles. If the QRSs originate from different foci, each QRS will look different and that is called "multifocal PVCs." If they originate from the same foci, the QRSs will look the same and that is called "unifocal PVCs." Sometimes you have normal sinus, then a PVC--bigeminy.
Sometimes you have 2 normal sinus, then a PVC--trigeminy.
Sometimes you have normal sinus, then two PVCs in a row, then normal sinus--couplet (of PVCs).
If you have 3+ PVCs, that's considered ventricular tachycardia.
rate: anything
rhythm: can be regular, can be irregular, can even be regularly irregular
P-wave: usually hidden under the QRS
P-R: nonexistant (duh ^^)
QRS: wide and distorted
Causes: stimulants, amniophylline, epi, dig, electrolyte imbalance, hypoxia, fever, stress. Treatment: remove stressor--if hypoxic, give oxygen, if fever, give tylenol, if stress, reduce stress, if stimulants, excrete stimulants, etc. Give B-block, Ca2+ block, procanimaide, amiodarone.
Ventricular tachycardia: 3+ PVC's. One type of V-tach is Torsades de Points, which is a polymorphic VT and a prolonged QT interval. V-tach can quickly degenerate into V-fib.
rate: 250+
rhythm: regular
P-wave: invisible
P-R: nonexistant (duh^^)
QRS: varies
Causes: Prolongued QT (sometimes caused, ironically, by antiarrhythmics), genetics, heart damage (MI/CAD), CNS disorders/electrolyte imbalance.
Treatment: If pt has a pulse: procainamide, sotolol, amiodarone, implantable cardioverter-defibrillator
If a patient does not have a pulse: CPR, D-fib. If d-fib unsuccessful, follow with vasopressors (epinephrine), antidysrhythmics (amiodarone).
Ventricular fibrillation: tiny squiggly line. NO PULSE. CPR, D-fib. If d-fib unsuccessful, follow with vasopressors (epinephrine), antidysrhythmics (amiodarone).
Pulseless Electrical Activity: PEA is where you see electrical activity on the screen, but there is no pulse in the patient. It is most commonly seen after D-fib (for v-fib or hemodynamically unstable v-tach), and the only thing you can do for this patient is CPR and try to figure out what is causing the PEA. Causes include: The H's and the T's (see below)
- hypovolemia (give volume, obviously: PRBCs, D5W or .9NS wide open, elevate the legs, do whatever you need to do to make the systemic volume go up--remember pressors only work if there is adequate volume in the body already)
- hypoxia (O2, really sucks if it's carbon monoxide poisoning...)
- met. acidosis (bicarb, regular insulin with D20W, potassium if the etiol is hypokalemia--highly unlikely, I know--and intubate that person because you better believe his ventilatory drive is in the toilet with respiratory fatigue from trying to blow off CO2.)--Yeah, I know this is neither an H or a T. Whatever. It was in my textbook.
- hypokalemia (give potassium IV DILUTED)
- hypoglycemia (D20W)
- hypothermia (warm .9NS)
- toxins (antidotes, dialysis, chelation)
- cardiac tamponade (decompress the pericardium--no, not you, the doctor)
- thrombosis (suck that sucker out--not you, the doctor)
- tension penumo (insert chest tube)
- trauma (fix it, whatever it is)
Sudden Cardiac Death: if I remember correctly, usually happens to young people who were just really active sending them into Vtach or V-fib, and you just need to do CPR and D-fib until help arrives with epinephrine and amiodarone.
Prodysrhythmia: this is when antidysrhythmic medication like dig, or amiodarone causes the same dysrhythmias for which they were prescribed. Yup. It happens. I don't know how to treat it directly--that is the doctor's job to figure out. I just treat according to what the EKG looks like until the doctor figures it out.
Asystole: CPR, treat the cause. Epinerphine, vasopressin. Causes include: hypoxia, acidosis, electrolyte imbalance, drugs, hypovolemia, cardiac tamponade, tension pneumo, MI, hypothermia, trauma.
But basically, I hope you started to see a pattern here: Any time there's an inconsistent rhythm you were given an antiarrhythmic like amiodarone or ibutilidem. Any time the heart was going too slowly, there was atropine. Any time the heart was going too fast, there was B-blocks, Ca2+ channel blocks, dig. Any time the patient was hemodynamically unstable but still had a pulse, cardioversion. Once there was loss of consciousness but still electrical signal, CPR, then d-fib, epi, and amiodarone--except with PEA, where you have to figure out all the hypos or to toxins, thrombosis, tension pneumo, or trauma.
CARDIOVASCULAR SYSTEM DISORDERS
btw, Khan Academy (which you should all donate to), has free tutorials and NCLEX-RN questions on this cardiac dysrhythmias. Quick repost of lab values:
ESR: 1-13 (the Mayo Clinic says 1-22**)
C-reactive protein: risk for CAD normal <1; average 1-3; high risk >3
PTT: 16-40; aPTT 1.5-2.5X norm
PT/INR: 11-12.5/0.7-1.8 (2-3 on coumadin)
BUN: 10-20 Video on BUN here
Creatinine: 0.6-1.2
LFTs:
- Cholesterol <200
- Triglycerides <150
- LDL <130
- HDL <65
- Albumin: 3.5-5
- AST aspartate aminotransferase and ALT alanine aminotransferase 0-35 (signs of hepatitis)
Video on liver function tests here - ALP alkaline phosphatase 30-120 (biliary tree obstruction)
BNP: no failure <100, possible failure <300, failure >300 (300 mild, 600 moderate, 900 severe)
Creatinine phosphokinase MB (CK-MB): <5% (<25 IU/L)
Troponin: <0.2
Here are a few ECG variations you should remember for Acute Coronary Syndrome:
 |
| MedSurg by Lewis Dirksen Heitkemper Bucher 9th edition, page 806. |
Hypertension: Ok, so hypertension can occur because of multiple reasons (pheocromocytoma, renal failure, heart failure, bad diet, and the race most affected is African Americans, especially the men) but whatever the case may be, in the end you need to do the same basic things: eat a heart healthy diet (low sodium, low fat), exercise. If your hypertension is bad and has caused damage to your kidneys, AND/OR your hypertension is now worsening because your kidneys have conked out on you (remember, you can tell that a person is in renal failure if the creatinine>0.6-1.2; and especially if both Creat:BUN are elevated but the ratio is still 1:10 to 1:20, so like Creat 20:BUN 300.), you need to offload that fluid before you drown (pulmonary edema) with ACE-inhibitors and diuretics, and you need to help your poor, beat up heart (Ca2+ blockers, B-blocks, dig) beat better.
I'll do a review of these medications in another post.
Angina: comes in 3 forms:
1) stable (triggered only by exertion and stress)
2) unstable (fatty deposits rupture/blood clots form, suddenly blocking a narrow artery=suddden decrease in blood flow) that is not relieved by medications
3) variant aka Prinzmetal, very rare, and is a spasm in the coronary artery.
Risks are (of course) family history, smoking, hyperlipidemia (cholesterol>200; Triglyc>150, LDL>130, HDL>65), which often accompanies sedentary lifestyle and obesity, and diabetes.
If a patient presents to the ER in acute onset of angina (s/s of acute coronary syndrome), assess the patient for location of pain, character of pain, duration of pain and whether it was relieved with rest or nitro on scene, and what precipitated the onset of angina (and of course eliminate those triggers to avoid addition attacks while in the ER).
then, administer MONA in this order:
1) Oxygen (ABC)
2) Nitro
3) Aspirin
4) Morphine
and then, 5) thrombolytics.
and, if necessary, prepare for transport to the cath lab or surgery. If the patient is stabilized and the doctor feels that it is unnecessary to do PCI, then anticipate beta blockers, aspirin, nitrates, statins, Ca2+ channel blockers, and angiotensin converting, enzymes.
In the real world, you may give MONA immediately without getting an ECG, because the sooner oxygen and blood flow is restore, the more likely you are to recover from ischemia and not progress to injury or infarction, but for the purposes of the NCLEX, you always assess first--it is NCLEX world in perfect harmony, and the patient will not die before you finish your assessment.
Cardiac catheterization: There are two types of cardiac cath for ACS: coronary angioplasty (a balloon is inflated at the site of blockage and mashes the fat against the wall to create a bigger opening), and coronary stent (the same thing as an angioplasty, but you leave behind a fine mesh to keep the fat from collapsing in as soon as you back out of there).
The main things you need to remember as a nurse for cardiac cath is: it's percutaneous (percutaneous coronary intervention), may require dye (check for shellfish allergy--although, many of my doctors have said that the correlation between shellfish allergy and dye allergy is a debunked myth, so who knows), so you will need to:
- NPO
- verify consent
- shave prep (always a trick question whether to shave or to cut hair at the site with scissors to microcuts and prevent infection. I've never known sources to agree--it's like, whatever, you're going to use betadine/chlorhexadine in a second, who gives a fuck.)
- explain dye--"you may feel flush and taste a metallic tang," and check for allergies
- mark baseline pulse
Your main concern is hemorrhage through the femoral artery (and it has to be the artery because you're going into the coronary arteries and that's the only way to them--it's not like you can go through the ICV and thread through the alveoli and back out into the aorta), so:
- APPLY PRESSURE FOR 15 FULL MINUTES (at least, especially if PT>12.5/INR>2-3), oftentimes you'll use a sand bag to maintain pressure, and KEEP THE LEG EXTENDED--in fact NO HIP FLEXION IN BED for 4-6 hrs.
- monitor hemorrhage q 15 min for the first 4 hrs, then 30 minutes, then hourly, etc.
- monitor neurovascular q 15 min for the first 2 hours, then 30 minutes, etc.
- increase fluids (for hypovolemia, and to wash out dye)
Anticipate the doctor will put the patient on the same medications as for a patient with stable angina without PCI, that is: beta blockers, aspirin, nitrates, statins, Ca2+ channel blockers, and angiotensin converting, enzymes. You'll have to teach the patient to avoid the valsalva maneuver, avoid stress/sudden bouts of physical activity (ESPECIALLY in the cold--Jesus. All of those people who suddenly decide that they're going to shovel their house out of a blizzard and end up dying of heart attacks on their sidewalk), rest after eating (especially hard to digest things, like steak), and stop smoking. Exercise LIGHTLY--seriously, walking is enough--and eat a heart healthy diet. (Like, duh.)
So, with the medications you have to teach:
nitro--SIT YOUR ASS DOWN, take with onset of angina SL q 5 minutes up to 3 times. Call 911 if it's not relieved after the first tablet. Keep the nitro in a dark, dry container out of the light and away from heat, and replace q 6 months even if you've never used it--don't be cheap about this medication. If you're taking it and you don't get a headache, maybe the nitro isn't working. If you're taking nitro on a daily basis (as a cream or a patch) you have to use it for ONLY 12 hours a day (applying it in the morning) and wash it off for the other 12 hours to prevent developing a tolerance. And do not take it if you are on a sildenafil (Viagra) because your blood pressure will bottom out and you will die. I mean, be nicer than that, but make sure that the patient gets that this is serious.
Ok, so you've had angina, and a cardiac cath, and you're still eating McDonalds, or you haven't given up your job as a top litigator and then you decided to go shovel your house out in the middle of a blizzard and you've had a full on grade A heart attack and given yourself a massive myocardial infarction. Maybe you went into V-fib, had to be D-fibbed and had someone pound on your chest and break a few ribs the whole way from your house in the back of an ambulance to the hospital, where they discovered that a piece of artherosclerotic gunk broke off in spite of the coronary stent, and got lodged in your left coronary artery. They cracked you open, did a CABG on you, and now you're in ICU, in extreme pain (fun fact: diabetics, due to diabetic neuropathy, may not report pain), and your ECG is showing simultaneous ST-segment elevations and T wave inversion. (Which reminds me, I really have got to exercise today...)
Myocardial infarction: s/s: severe chest pain (or not, with diabetes, women or elder patients) unrelieved with nitro or rest that crushes and radiates to jaw, left arm, neck, back, etc. Diaphoresis, N/V anxiety, ECG shows tachycardia/dysrhythmias c possible ST elevation (STEMI) and/or T inversion, hypotension + dyspnea. Expect troponin>0.2, CK-MB>3, LDH (lactic acid dehydrogenase) >140-200,
Nursing goal: Rest the myocardium and preserve heart muscle.
MONA:
Immediately: Oxygen, nitro, aspirin, morphine, streptokinase or alteplase (within 6 hours), amiodarone, calcium channel blockers.
Later: stool softeners + bedside commode, promote self care and exercise but stop if fatigued or angina occurs, heart healthy diet, stress management, smoking cessation.
Discharge medication: heparin, aspirin, warfarin, enoxaparin, clopidogrel (antiplatelet), metoprolo, diltiazem (Ca2+), nitro, simvastatin (antilipidemia).
The result of a myocardial infarction is heart failure.
Heart failure: A chronic condition where the heart is unable to meet the body's oxygen requirements, and is often accompanied by fluid overload/inadequate tissue perfusion + fluid retention due to decreased renal circulation. Depending on what caused the heart failure (cor pulmonale, which coronary artery was blocked, kidney failure, hypertension, etc.) there may be L.S. HF (symptoms are related to decreased systemic/pulmonary circulation, i.e. elevated PAWP, pulomonary edema and paroxysmal nocturnal dyspnea, low O2 sat), or R.S. HF (symptoms related to systemic congestion, i.e. acites, hepatosplenomegaly, dependent edema + fluid weight gain, elevated CVP, JVD, anorexia/vomiting)
Ok, wait, but what is the PAWP and the CVP? I ask, because I know it has to do with catheters measuring pulmonary artery wedge pressure (PAWP) and central venous pressure (CVP), but that's about all I remember. So, let's take a side trip into HEMODYNAMIC MONITORING. If you already got the theory, here's the hemodynamic values you should know:
CVP: 1-8mmHg
PAWP: 4-12 mmHg
Cardiac output 4-8L/min = Stroke volume x Heart Rate
Mean arterial pressure 70-105 mmHg = [systolic + 2diastolic]/ 3
Systemic vascular resistance 1970-2390 gynes/sec/cm^-5= [(MAP-CVP) x 80]/ CO
Arterial hemoglobin saturation 95-100%
Mixed venous hemoglobin (SCVO2): 60-80%
CVP: 1-8mmHg
PAWP: 4-12 mmHg
Cardiac output 4-8L/min = Stroke volume x Heart Rate
Mean arterial pressure 70-105 mmHg = [systolic + 2diastolic]/ 3
Systemic vascular resistance 1970-2390 gynes/sec/cm^-5= [(MAP-CVP) x 80]/ CO
Arterial hemoglobin saturation 95-100%
Mixed venous hemoglobin (SCVO2): 60-80%
If you didn't take the side trip, basically, you need to know that elevated levels of CVP (>8)and PAWP (>12) mean that the heart is (for whatever reason) unable to pump blood efficiently. In the case of heart failure, it's because of heart failure (duh).
Treatment of heart failure= pump it, park it, pee it=focuses on decreasing fluid volume overload and helping the heart to pump more efficiently (inotropic medications)/decreasing systemic vascular resistance.
Medication for inotropic (pump it): digoxin
Medications for decreasing systemic vascular resistance (park it): B-block, Ca2+ ch. block, nitrates/hydralazine, nesiritide, milrinone, dobutamine.
Medications for decreasing fluid (pee it): ACE inhib, ARB, diuretics
Coronary artery bypass graft (CABG): usually requires an open chest surgery with bypass (ECMO). Your job as a nurse is to:
preoperatively: VS, assessment, HX. support (psych and anxiolytics), teach the family and patient to anticipate intubation, IV lines, foley, arterial line, chest drainage tubes.
postoperatively: hourly assessement for first 8 hours of complications:
- vitals, neurological (pupils, reflexes, Glasgow)
- cardiac: CVP, PAWP, ECG, sounds, increased bruising, etc., peripherals
- resp: ventilator settings
- renal: I&O, electrolytes, urine specific gravity
- pain: location, type, intensity, onset
DVT: usually caused by increase in thrombi formation (think estrogen in pregnancy or contraceptives, or long term immobility from injury, immobility, or age). You'll see a red, hot swelling of one limb, that may be bumpy, knotty, and shiny (edema leaking through). You may see a venous ulcer (usually medial side of the leg at the ankle or above). It is best prevented by ambulation, weight loss, wearing supportive antiembolitic socks, and elevating the lower extremities and not crossing your legs, and preventative SQ heparin. It is diagnosed with an MRI, Spiral CT, U/S, and then treated with heparin (PTT 60-100) and warfarin (INR 2-3), alteplase, elevating the extremity, applying warm, moist compress, and being vigilant for s/s of PE, stroke, or MI. Otherwise, sclerotherapy, ligation and stripping, or thermal ablation may be necessary.
Peripheral artery (occlusive) disease (PAD): Peripheral arterial disease is just a buildup and consequential narrowing of arteries. It is a significant risk for future major coronary events--note the name "peripheral artery disease" is misleading because atherosclerosis can happen all over the body, such as in the heart (CAD) or in the brain (cerebrovascular disease). As such, the risk factors of PAD is the same as those for CAD, which are, high cholsterol >200, high triglycerides >150, and elevated CRP >3, smoking, diabetes, etc. S/s include: intermittent peripheral claudication pain that resolves with rest (because decreased blood flow will exacerbate the removal of lactic acid), and calf muscle atrophy, and shiny skin with hair loss, paresthesia, and thick toenails (signs of decreased oxygen and nutrients reaching cells), and may lead to leg ulcers.
Leg ulcers are another thing that I found really confusing because it's never really well explained. I'm still not good at it, but as I've said before, I've accepted that there are many things that will make sense to me, and that I will learn after I've passed the NCLEX. To see a quick differentiation of leg ulcers, take a look here.
Along the same vein, there is a similar disease called...
Thromboangiitis obliterans aka "Buerger's disease": a disease that causes repeated inflammation of the blood vessels of the extremities, resulting in idiopathic thrombosis and occlusion. This also has the symptom of intermittent claudication, inflammation due to clots, and cold skin that is relieved by rest, smoking cessation, avoiding caffeine, and avoiding constrictive clothing or the cold. If it is prolonged open sores may occur on the fingers and toes that require amputation.
To make things more confusing, there is another similar disease (that actually popped up on my NCLEX-PN as the final question) called...
Raynaud's syndrome: a disease that causes vasospasms/constriction of the arteries due to exposure to cold and stress. These may lead to ulcerations of the fingertip, so the patient should wear extra clothes in the cold, but make sure that the clothes are not restrictive. Smoking cessation, and limiting caffeine intake is also suggested. You could also administer nifedipine. Nifedipine would NOT work with thromboangiitis obliterans because there is inflammation and thrombosis involved.
Structural Cardiac Disorders
Valvular disorders: valve disorders are mostly cases of stenosis which makes it difficult for the heart to eject blood, but also, allows for backflow (leaking) back into the chamber that was just pumping. Just remember the side each valve is located (R: tricuspid, R pulmonary, AV; L: mitral, aortic, AV). Murmurs are just the turbulence of blood sloshing around erratically because of the stenosis or prolapse. Mostly it leads to heart failure. The only treatment is surgery for replacement, which will require warfarin for life if it's mechanical, and immune suppressants if biological (but warfarin only for 3 months). If you have an autologous fancy, valve, you won't need either except in the immediate postoperative. All of the valve surgeries will require prophylactic antibiotics for any further procedure to prevent infective endocarditis.
Aortic aneurysm: usually caused by congenital connective tissue disorders, but also from infection and atherosclerosis. An aortic aneurysm greater than 5 cm requires surgical intervention. Usually a patient doesn't even know he has an aortic aneurysm. He may complain of:
- thoracic pain, dyspnea, hoarseness, cough, and dysphagia (remember, the larynx, pharynx, esophagus, trachea, are all in the mediastinum with the aorta and the heart)
- lower aneurysms (remember, the abdominal aorta is still part of the aorta) may cause abdominal pain, persistent or intermittent low back or flank pain, and you might actually be able to see a pulsating abdominal mass
Your job as the nurse is to:
Preoperative: maintain systolic between 100-120 with beta-blockers, antihypertensives. Continuous nipride might be prescribed, and to be vigilant for signs of rupture (sudden, intense pain with rapid BP drop). Also, you'll have to care for the patient during CT scans, MRIs, X-ray, and ultrasound.
Postoperative--basically the same as preoperative because now, instead of an aneurysm, you've got a line of sutures holding the aorta together. Freaking hell! And of course, infection.
SHOCK
Ah, shock. So many versions. So confusing. I'd encourage you to make a chart in the end to get an overview, but I'm just going to talk about each separately. I personally found this Khan Academy video very helpful. There is also a collection of review questions from Khan Academy. As I said before, I highly suggest donating to them since they provide excellent education for free, which helps those who come from socioeconomic hardship to have the same education someone of means might get from a private school. Here's a great story showing that.
First off, shock is any situation where there is decreased tissue perfusion and impaired cellular metabolism, resulting in cell starvation. There are 4 main categories: cardiogenic, obstructive, hypovolemic, and distributive.
Cardiogenic shock, obstructive shock, and hypovolemic shock are the ones you'll most see on TV. They're slightly difficult to tell apart because they all have some form of decreased cardiac output, and in response the blood vessels constrict in attempt to increase blood return to the heart. In addition, all three have decreased mix oxygen content (MVO2) because the body's cells are desperately trying to pull as much oxygen out as possible, resulting in a low oxygen content in the blood returning to the heart. They deviate when it comes to preload levels. In cardiogenic and obstructive shock, you'll see an increased PAWP>12 (remember, this measures how much pressure is in the ventricles at the end of diastole) because the ventricles are unable to properly eject blood out of the heart either because the heart is damaged (like from an MI) and unable to pump (cardiogenic shock), or because there's an obstruction (like an aortic stenosis or cardiac tamponade) preventing the blood from flowing (obstructive shock). In hypovolemic shock, there simply isn't enough volume in the body to properly fill the ventricles (because of dehydration or hemorrhage) resulting in a lower PAWP<4. With cardiogenic shock you have to fix whatever damage there is to reestablish proper circulation, and with obstructive shock you have to either unplug the thrombosis or open the stenosis. With hypovolemic shock you have to fix the source of the bleed, or simply refill the body with blood components and/or fluid. The emergent steps to stabilize a patient (for surgery): 1) Establish airway, give O2, and 2) improve circulation and contractility with epinerphine (vasopressor) and IVF, and 3) then repairing the problem.
Distributive shock: Neurogenic, septic, and anaphylactic
Neurogenic shock, which occurs when the spine is injured, causing an impairment in sympathetic response. Neurogenic shock is the only shock that results in a BRADYCARDIA and simultaneous decrease in nervous system tone (blood vessel dilation). So, the spine is injured, HR drops, causing cardiac output to decrease (SV x HR= CO<4L/min), and the blood vessels aren't constricting. PAWP isn't really affected even though there is decreased vascular resistance. Mixed oxygen saturation should be low because the blood is traveling slower so the surrounding tissue has more time to absorb O2. Treatment should be to maintain BP: pressors, IVF, atropine (blocks the parasympathetic nervous system=stops rest and relax signals to increase the heartrate).
___________Detour into neuro for a second: SCI
With SCI, if the injury is above T6, there is a risk of autonomic dysreflexia should the patient experience bowel impaction, bladder distension, triggering of pressure points, ulcers, or pain. Autonomic dysreflexia is a life-threatening syndrome of sudden, extreme hypertension, with bradycardia (30-40bpm). Other s/s: H/A, piloerection, flushing above the level of the injury, blurry vision, nasal congestion, and nausea.
The order of nursing actions is:
- High fowlers (I know, your first instinct is to roll that person over and try to un-impaction him, but, don't, cause that may not be the problem. Putting the person in high fowlers buys you time to assess the causation)
- (have someone else) alert the physician
- determine and remove causative stimuli--also remove anything that may cause more stimuli to the patient
- give medications (lidocaine, to help with digital fecal removal and/or bladder cathing, a-blockers, and Ca2+ channel blockers)
- teach bowel and bladder management
________________________End detour
Septic shock and anaphylactic shock are another couple that have strong similarities. Septic shock and anaphylactic shock both have immune mediated systemic vasodilation, which causes edema (resulting in decreased circulating volume, and makes it more difficult for O2 to diffuse from the blood vessels to the tissues). In both, PAWP is marginally decreased, but not by much, if at all. The treatment for septic shock is 1) (Airway, Breathing) ventilation; 2) (circulation) IVF, pressors, 3) treat the source with blood cultures and ABX (desire CRP<1, ESR <20-25 = decreased inflammation, and decrease bacterial count), and the treatment for anaphylactic shock is 1) establish airway with ventilation, 2) maintain BP with epinephrine (and open airway) and IVF, and 3) continue to reverse the allergic reaction with benadryl.
There's also something called dissociative shock in which hemoglobin doesn't release O2. There are 2 causes of dissociative shock. The first is: sometimes a person has red blood cells where the iron in the hemoglobin is Fe3+ instead of Fe2+. Fe3+ (ferric ion=methemoglobinemia) causes Fe2+ hemes to increase in ferrous ion oxygen binding. This is caused by nitrates, especially antibiotics, (such as TMP/SMX, and dapsone), or anesthetic (like benzocaine), or pesticides. Neonates are especially vulnerable to methemoglobinemia because they're missing an enzyme that converts Fe3+ to Fe2+. Treatment of methemoglobinemia is IV methylene blue, which causes Fe3+ to be converted back to Fe2+. The other cause of dissociative shock is CO (carbon monoxide) poisoning which has a 100X greater binding ability to hemoglobin than O2. It causes a change in shape of the hemoglobin, preventing their release. The cause of CO is carbon combustion, like a fire burning stove. Treatment is oversaturation with O2 in a barometric chamber.
No comments:
Post a Comment