I promised I would get to an ABG Tutorial, so, I'm finally doing it.
What's the point of ABGs?
The human body functions in a narrow pH window of 7.35-7.45--but what does that mean? When we think about the human body, or any living thing, really, we should be thinking about enzymes--little super efficient protein clumps that help to speed reactions that allow us to exist as large, billion celled complex creatures. Those enzymes are very sensitive to environmental changes. For example, if you heat or freeze them, like with a fever, or with hypothermia, they'll fall apart and stop working, and then the person dies. The physiologic pH range necessary to prevent the enzymes in the human body from denaturing (coming unwound and falling apart into bits) and inactivating, is between 7.35 and 7.45. If you party a little too hard and throw up for hours (losing acid from your stomach), or eat some bad shellfish while you're in Cancun and have 25 sessions of diarrhea in a day (losing a lot of base), or if you have COPD, so you can't breathe out the carbon dioxide (holding on to acid), or if your bother tackled you too hard playing football and you tore your ACL and you're hyperventilating because you're in pain (blowing off all the acid), you could shift toward an acidic blood level (<7.40) or basic blood level (7.40<). Luckily, our bodies have safety mechanisms built into place to compensate for those kind of pH shifts.
Where did the acids and bases come from to begin with?
Acid is a natural byproduct of cellular respiration. You can learn more about it with this Youtube Video by Eric Strong, MD., but let me just show you this equation:
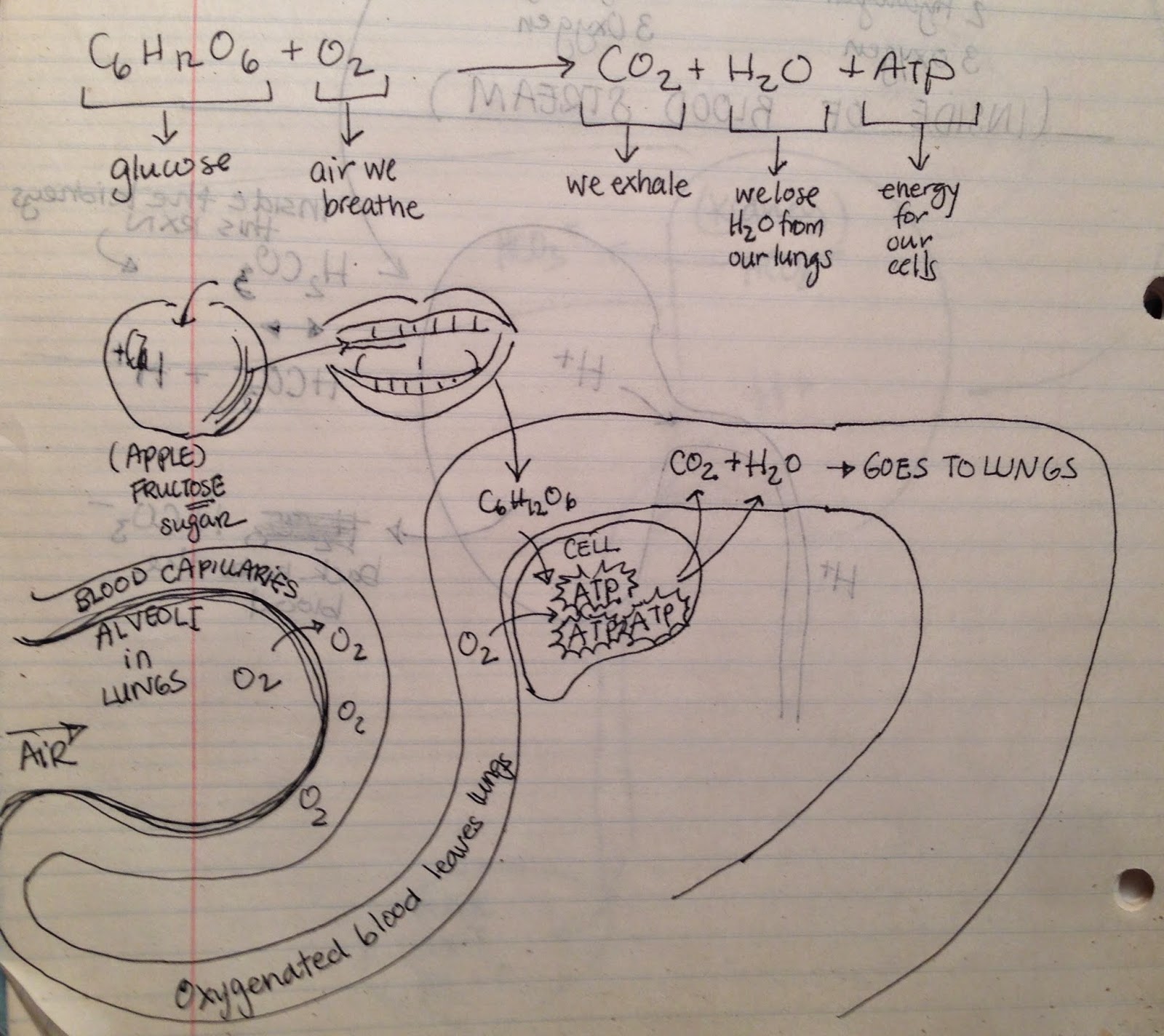
Sugar = C6H12O6
Oxygen = O2
Carbon Dioxide = CO2
Water = H2O
Energy = ATP
Sugar (from food) + Oxygen (from lungs) go into the blood and into the cells
The cell metabolizes the sugar and oxygen and releases Carbon Dioxide + Water + ATP (which gets used by the cell). The CO2 and H2O goes into the blood stream:
Carbon Dioxide + Water --> Carbonic Acid --> Protons + Bicarbonate
(If you are curious as how these components all fit together in cellular respiration, read this next post on cellular respiration, or watch this great Khan Academy video on Citric Acid and Krebs Cycle. But it's not necessary to understand all of this to understand acid-base.)
In chemistry, we learned that protons are just a hydrogen stripped of an electron. They look like this: H+. We also learned that the definition of an acid is the ability for a substance to give up a proton. You might remember, also, that bicarbonate (HCO3-) is a weak base because it only has the ability to pick up a single proton. In the human body, once sugar and oxygen have broken down into H+ and HCO3-, they get pumped in the blood to the kidneys where the protons are urinated out, and the kidneys preserve the HCO3- as a "buffer" or a substance that prevents pH from shifting because it can easily pick up, carry, and later let go of H+'s. This entire equation:
CO2+H2O<-->H2CO3<-->H+ + HCO3-
is the buffer that prevents our blood from swinging from acid to base (or vice versa) and killing us.

There are two main hurdles to get over when thinking about Arterial Blood Gases (ABGs). The first is, memorizing ranges. If you're like most nursing students, you hate memorizing ranges. You can memorize something like the back of your hand, walk away for a few months, and not even realize you forgot what you forgot. We just went over it with our NCLEX review class and I found myself stuttering a little with the ranges, and then having to double check to see if I got the compensation correct, so, I need the practice, too, and I am not claiming to be perfect at these.
Bicarbonate is chemically written as HCO3− but I'll write it as HCO3-, since it's easier to type.
The second hurdle regarding ABGs is incorporating metabolic or respiratory into the picture. I'd like to disabuse you of the concept that metabolic means a kidney problem, and respiratory means a problem with the lungs. Yes, on one hand, metabolic conditions are influenced by the bicarbonate concentration, which is largely conserved by the kidneys, however, the kidneys can be the origin of the bicarbonate imbalance, or it can be a compensatory mechanisms. Similarly, if there is a change in CO2, it can be because there is something wrong with the lungs, or, it can be that the lungs are compensating for a problem somewhere else in the body. As with all other conditions of the body, there is overlap, so I challenge you to approach ABG's with a bird's eye view. I'll revisit this concept after we've nailed down a few basics.
What's the point of ABGs?
The human body functions in a narrow pH window of 7.35-7.45--but what does that mean? When we think about the human body, or any living thing, really, we should be thinking about enzymes--little super efficient protein clumps that help to speed reactions that allow us to exist as large, billion celled complex creatures. Those enzymes are very sensitive to environmental changes. For example, if you heat or freeze them, like with a fever, or with hypothermia, they'll fall apart and stop working, and then the person dies. The physiologic pH range necessary to prevent the enzymes in the human body from denaturing (coming unwound and falling apart into bits) and inactivating, is between 7.35 and 7.45. If you party a little too hard and throw up for hours (losing acid from your stomach), or eat some bad shellfish while you're in Cancun and have 25 sessions of diarrhea in a day (losing a lot of base), or if you have COPD, so you can't breathe out the carbon dioxide (holding on to acid), or if your bother tackled you too hard playing football and you tore your ACL and you're hyperventilating because you're in pain (blowing off all the acid), you could shift toward an acidic blood level (<7.40) or basic blood level (7.40<). Luckily, our bodies have safety mechanisms built into place to compensate for those kind of pH shifts.
Where did the acids and bases come from to begin with?
Acid is a natural byproduct of cellular respiration. You can learn more about it with this Youtube Video by Eric Strong, MD., but let me just show you this equation:
Sugar = C6H12O6
Oxygen = O2
Carbon Dioxide = CO2
Water = H2O
Energy = ATP
Sugar (from food) + Oxygen (from lungs) go into the blood and into the cells
The cell metabolizes the sugar and oxygen and releases Carbon Dioxide + Water + ATP (which gets used by the cell). The CO2 and H2O goes into the blood stream:
Carbon Dioxide + Water --> Carbonic Acid --> Protons + Bicarbonate
(If you are curious as how these components all fit together in cellular respiration, read this next post on cellular respiration, or watch this great Khan Academy video on Citric Acid and Krebs Cycle. But it's not necessary to understand all of this to understand acid-base.)
In chemistry, we learned that protons are just a hydrogen stripped of an electron. They look like this: H+. We also learned that the definition of an acid is the ability for a substance to give up a proton. You might remember, also, that bicarbonate (HCO3-) is a weak base because it only has the ability to pick up a single proton. In the human body, once sugar and oxygen have broken down into H+ and HCO3-, they get pumped in the blood to the kidneys where the protons are urinated out, and the kidneys preserve the HCO3- as a "buffer" or a substance that prevents pH from shifting because it can easily pick up, carry, and later let go of H+'s. This entire equation:
CO2+H2O<-->H2CO3<-->H+ + HCO3-
is the buffer that prevents our blood from swinging from acid to base (or vice versa) and killing us.
There are two main hurdles to get over when thinking about Arterial Blood Gases (ABGs). The first is, memorizing ranges. If you're like most nursing students, you hate memorizing ranges. You can memorize something like the back of your hand, walk away for a few months, and not even realize you forgot what you forgot. We just went over it with our NCLEX review class and I found myself stuttering a little with the ranges, and then having to double check to see if I got the compensation correct, so, I need the practice, too, and I am not claiming to be perfect at these.
Here are the lab values you need to memorize. Sorry, there's no getting around it.
PaO2 80-100 mm Hg
SaO2 95-100%
pH 7.35-7.45
PaCO2 35-45 mm Hg
HCO3- 22-28 mEq/L
Bicarbonate is chemically written as HCO3− but I'll write it as HCO3-, since it's easier to type.
The second hurdle regarding ABGs is incorporating metabolic or respiratory into the picture. I'd like to disabuse you of the concept that metabolic means a kidney problem, and respiratory means a problem with the lungs. Yes, on one hand, metabolic conditions are influenced by the bicarbonate concentration, which is largely conserved by the kidneys, however, the kidneys can be the origin of the bicarbonate imbalance, or it can be a compensatory mechanisms. Similarly, if there is a change in CO2, it can be because there is something wrong with the lungs, or, it can be that the lungs are compensating for a problem somewhere else in the body. As with all other conditions of the body, there is overlap, so I challenge you to approach ABG's with a bird's eye view. I'll revisit this concept after we've nailed down a few basics.
pH 7.35-7.45, PaCO2 35-45 mm Hg, HCO3- 22-28 mEq/L tells you the acid base status of the patient--in other words, if the blood pH is normal, too acidemic, or too alkalemic.
PaCO2 35-45 mm Hg tells you the patient's ventilation status. If this number is high, either your patient isn't breathing out the CO2 efficiently enough, or your body is creating a high concentration CO2 (from cellular respiration), or both.
PaO2 80-100 mm Hg, SaO2 95-100%, PaCO2 35-45 mm Hg together give you a picture of how well the patient is being oxygenated.
PaO2 80-100 mm Hg, SaO2 95-100%, PaCO2 35-45 mm Hg together give you a picture of how well the patient is being oxygenated.
For this post, let's just focus on acid-base part of the ABGs: pH, PaCO2, and HCO3-.
I'm sure you've seen a pH scale like this in your general chemistry class:
 |
| https://sciencesummative.files.wordpress.com/2013/01/ph-scale.jpg |
In your body, your blood should have a pH level between 7.35-7.45. Technically, anything above 7 is alkaline, so, our bodies are actually a little on the alkaline side, but, look, a pH of 7 is pure water, and 8 is seawater. Since our blood does have salt and other electrolytes in it, but it's definitely not as salty as seawater, it would make sense that it would fall somewhere between 7 and 8.
Let's just zoom in on the section we need:
 |
| http://image.slidesharecdn.com/07-140422135054-phpapp02/95/07-acid-base-disorders-8-638.jpg?cb=1398192734 |
Tip 1:
A caveat about the pH range of blood: just because the pH value is within that range, does not mean the blood isn't more acidotic or alkalotic. Perfectly balanced blood is 7.40, but that is just one point on the scale. In other words, if the pH is between 7.35 and 7.40, it is on the acidic side of normal, and if the pH is between 7.40 and 7.45, it is on the alkalotic side of normal. This comes into play with compensation.
Tip 2:
When looking at the paCO2 values and the HCO3- values, consider what those numbers mean. We know that the normal range for paCO2 is 35-45, so what does a paCO2 of 20 mean? 50? We know that the normal range for HCO3- is 22-26, so what does a HCO3- of 16 mean? What does a HCO3- of 30 mean?
Think about it in terms of water, cream and coffee. For argument's sake, let's say that the water has the same pH as our blood in perfectly balanced conditions: 7.40. Coffee is acidic. Cream is alkaline.
If I had a big tub of water, and I dumped in 50 cups of coffee, would that new mixture now be more acidic than plain water? Yes. If I could magically remove 30 of those cups of coffee, would it be more or less acidic than when it had 50 cups of coffee? It would be less acidic.
If I took a clean tub of water and dumped in 22 cups of cream. Would that be more alkaline? Yes. What if I added another 14 cups? Would it be even more alkaline? Yes. What if I only had 10 cups of cream in a tub of water? Would it be less alkaline than 30 cups? 22? cups?
Tip 3: Using the Tub of Water/ Coffee & Creamer Metaphor
Okay, so, remember, in our perfect world, the tub of water has exactly a 7.40, perfectly balanced pH.
Now, what if I had a clean tub of water and I dumped in 40 cups of coffee (remember, paCO2 is 35-45, so 40 is a nice number right in the middle). That water is acidic. You would expect the pH to drop under 7.35, yes? Now, what if I add 24 cups of cream (remember HCO3- is 22-26, so 24 is a nice number right in the middle). That base will neutralize that acid, so the pH would bounce back up to somewhere between 7.35-7.45. Yes? What if I accidentally add too much cream? What if I add like 40 cups of cream? That solution would be alkaline, yes?
So, yes, the substance in the patient's blood is an acid (paCO2) or a base (HCO3-) but always ask yourself, how does the paCO2 and the HCO3- relate to the blood pH?
Can a low CO2 (acid) level cause an acidic blood pH if the HCO3- is normal? No. That's not logical, you have too little acid and too much base.
Can a high CO2 level cause an acidic blood pH if the HCO3- is normal? Yes. It's like having a tiny bit of cream in a whole lot of coffee. Your drink will be very acidic.
Can a low HCO3- level cause an alkaline blood pH if the CO2 is normal? No, you have too much acid and too little base.
Can a high HCO3- level cause an alkaline blood pH if the CO2 is normal? Yes. It's like having 50 creamers in your coffee--you'd feel like you were drinking milk with a side of coffee.
Tip 4: Compensation
In order for the body to survive the body must either create more acid, or more base to bring the pH back into balance between 7.35-7.45. This process is called compensation. The body is only compensated if the pH is within normal range.
Tip 5: The body will initially compensate with the other system
Initial pathological problem: high HCO3- (too alkalotic/basic=too much cream)
Body compensates by: increase PaCO2 (by slowing down breathing to retain CO2=adding more coffee)
Initial pathological problem: low HCO3- (not alkalotic/basic enough=not enough creamer)
Body compensates by: decrease PaCO2 (by increasing respirations to blow off CO2=using a smaller volume of coffee)
Initial pathological problem: high paCO2 (too acidotic=too much coffee)
Body compensates by: increasing HCO3- (peeing out a lot of H+ and sparing a lot of HCO3-=adding a lot of cream)
Initial pathological problem: low paCO2 (not acidotic enough=too little coffee)
Body compensates by: releasing HCO3- (peeing out bicarbonate=only using a little cream)
The steps for determining uncompensated acid base:
1) Look at the pH. Is it greater than 7.45 (alkaline) or less than 7.35 (acidic)?
2) Look at the paCO2. Is it less acidic than normal <35? Or is it more acidic than normal >45?
Can the pH be explained by this?
3) Look at the HCO3-. Is it less basic than normal <22? Or is it more basic than normal >26?
Can the pH be explained by this?
Examples:
pH 7.3 (<7.35=acidotic)
paCO2 50 (>45=high concentration of acid)
HCO3- 24 (right in the middle between 22 and 26=normal level of bicarbonate)
This is uncompensated respiratory acidosis.
pH 7.5 (>7.45=basic/alkalotic)
paCO2 20 (<35 = low concentration of acid)
HCO3- 24 (right in the middle between 22 and 26=normal level of bicarbonate)
This is uncompensated respiratory alkalosis.
pH 7.3 (<7.35=acidotic)
paCO2 37 (between 35-45= normal carbon dioxide level)
HCO3- 15 (less than 22-26)
This is uncompensated metabolic acidosis.
pH 7.5 (>7.45=alkalotic)
paCO2 37 (between 35-45 = normal carbon dioxide level)
HCO3-30 (greater than 22-26)
This is uncompensated metabolic alkalosis.
(Note: Uncompensated metabolic unbalances are rare, and usually happen because mechanical ventilation is also occurring.)
If yes, is it greater than or less than 7.40? (Remember, even within normal range, it can still be on the acidotic or alkalotic side).
__________________________
Compensated or uncompensated refers to whether or not the pH is within normal range. If the pH is within normal range, the body has compensated. End of story.
If the pH is not within normal range, the body has not yet compensated.
The confusing part is whether something is totally uncompensated (meaning the body hasn't started to change respirations or HCO3- concentrations to correct the pH imbalance), or partially compensated. In my mind, if the pH isn't within normal range, it is impossible to tell with only one set of ABGs whether something is beginning to compensate or not. How can you tell a trend with just one data point? But, GENERALLY speaking, your lungs start to react toward acid base imbalances faster than your kidneys (takes a few days), so if both your lungs and your kidneys are functioning, you'll se shifts in your paCO2 first. You're definitely uncompensated if the pH is imbalanced, AND both the kidneys (HCO3-) and the lungs (paCO2) have wacky numbers. And, if on the next draw the parameter that doesn't match the pH is continuing to move in the opposite direction, the body is compensating, but has only succeeded in doing so partially. For example, if your body is in metabolic acidosis, and on the first draw your PaCO2 is 35, and on the second it is 30, then your PaCO2 is becoming "less acidic," so you are breathing harder and faster to blow off more carbon dioxide (acid) to help make your body less acidic. If anyone can give me an actual way of magically telling with one data point when all three values are out of whack whether or not that body is partially compensated or just totally uncompensated, I'm all ears. Until then, I'm sticking with my story.
_________________________
Treatment of
- respiratory acidosis is to improve ventilation to help the person blow off acid (CO2)=mechanical ventilation
- respiratory alkalosis is to retain as much acid (CO2) as possible = paper bag, anxiolytics, pain medications, etc.
- metabolic acidosis is to bind, excrete, or store the acid (H+) by treating the underlying cause (tx DKA, tx salicylate or ETOH poisoning, tx dehydration/diarrhea/starvation, tx renal failure, or give bicarbonate)
- metabolic alkalosis is to excrete the bicarbonate: mechanical ventilation to prevent patient from dying of suffocation, and balance the electrolytes. Wait until the kidneys have excreted the adequate bicarbonate. If in renal failure, use dialysis.
The ATI reviews have this cute little chart they pass out that I won't replicate, because I don't want them to sue me, but essentially it goes like this:
resp acidosis--naloxone
resp alkalosis--re-breather
met acidosis--diphenoxylate/atropine (to make you stop having diarrhea), and humulin R (regular insulin), but then they didn't follow up with adjusting for potassium imbalances, etc.
metabolic alkalosis--ondansetron (to make you stop puking)
The reason why I'm not totally sold on that chart is because it makes a lot of assumptions about the etiologies of each of those scenarios.
References:
http://www.ncbi.nlm.nih.gov/pubmed/10421978
http://www.nlm.nih.gov/medlineplus/ency/article/003883.htm
http://www.rmtcnet.com/resources/Recommended%20Best%20Practices%20for%20TCO2%20Testing%20and%20Sample%20Collection.pdf
http://www.anaesthesiamcq.com/AcidBaseBook/ab2_4.php
http://en.wikipedia.org/wiki/Bicarbonate
http://www.anaesthesiamcq.com/AcidBaseBook/ab2_4.php
http://en.wikipedia.org/wiki/Bicarbonate
No comments:
Post a Comment